
Editor: Predrag M. Maksimovich, MD, DDS, ENT.
In this Online Journal we will publish various articles, comments, letters, etc in several languages. Where possible, translation to English will be provided.
All Medical Professionals visiting these pages are urged to contribute.
Materials should be sent to our e-mail address in .htm, WP6.0 or WFW 6.0 formats while the pictures should be in .jpg and .gif.
All comments, letters, suggestions are welcome.
![]()
Suppurative Otitis Externa
Diferrential Diagnostical Problems
Infections of Pterygomandibular Space - Differential Diagnostical Problem
Dundjerovic T, Mesterovic M, Jovanovic M, Buta S,
Maksimovic P.
Head and neck infections are one of the current problems in maxillofacial surgery. The occurrence of odontogenic abscess in pterygomandibular space is comparatively rare.
The authors report two patients with atypical symptoms. In both cases the presenting symptom was a firm, tender swelling of parotid region of the affected side with trismus. One of the patients had an abundant suppuration from the external auditory canal of the same side. First findings indicated toward a purulent otitis. After an otomicroscopic aspiration and finding of a fistulous oppening in the external auditory canal with intact tympanic membrane, an acute parotitis with spontaneous drainage of a parotid abscess was suspected. Despite a massive antibiotic treatment according to antibiogram, and in one patient after the incision, the symptoms persisted. After further examinations - orthopantomography and ultrasonography of the parotid region, the presence of a pterygomandibular abscess of dentogen origin was established. Extraoral incision of the abscess with extraction of the tooth (gangrenous maxillar third molar) was performed. Postoperative course was normal and complete healment ensued. The authors with this paper wish to point out the importance of the team work of the otorhinolaryngologist, maxillofacial surgeon and radiologist in differential diagnostics of the rare localizations of head and neck infections.
Differential Diagnosis of Suppuration from the External Auditory Meatus
Mesterovic M, Dundjerovic T, and Maksimovic P.
Authors present two patients with suppurations in the external auditory meatus which were treated conservatively and surgically under the diagnosis Otitis media purulenta. Because of the unsatisfactory effects of the prescribed therapy further investigations were conducted. The first patient had a long standing purulent secretion from his right external auditory meatus. Radical explorative mastoidectomy performed after extensive clinical otorhinolaryngological examinations, standard X rays and audiological tests showed no signs of the inflammatory middle ear process.However, a fistulous opening was observed at the anterior meatal wall.Additional tomography and CT scanning showed a malunited fracture of the mandibular collum with existing osteomyelithic focus, obviously a consequence of an old fracture. Surgical extirpation of bone fragments with condylectomy was performed. Additional therapy with hyperbaric oxygen was conducted. Postoperative course was normal.
The second patient was first seen with a large swelling in the right parotid region with massive suppuration from the external auditory meatus and trismus.
The initial suspition of acute purulent parotitis with with perforationt hrough the anterior wall of the external auditory meatus was confirmed during otoscopy. Our patient received massive doses of antibiotics and largepreauricular incision was performed but the drainage of the purulent collection was not obtained. Additional X ray and ultrasound examination revealed periapical process of the third maxillar molar tooth and purulent collection in the pterygomandibular space with lacunar purulent foci in the deep lobe of the parotid gland.
Head and neck infections are one of current problems in maxillofacial surgery.
In standard practice we encounter most frequently typical localizations and spreading pathways with typical causative microorganisms. Therapy is based on combination of antibiotic and surgical treatment. Most frequent infections in our region are of dental origin. A particular problem arises when the spreading pathways are atypical and symptomatology is hidden or bizarre. Diagnostical mistakes which lead to inadequate treatment by other specialists are then possible. Suppuration from the external auditory meatus in general implies an otogenic infection. Insufficiently precise anamnesis, clinical investigations and diagnostics with omission of appropriate specialists can lead to wrong kind of treatment, which in turn, further masks unclear symptomatology. Standard ENT examinations and explorative procedures in the temporal bone in diagnostically insufficiently clear cases should me managed in team effort with other specialties.
Material and Methods
We will report two patients with suppuration from the external auditory meatus, which were treated at first as a suppurative middle ear infection. Because of the poor effects of the prescribed therapy we performed more detailed roentgenographic and clinical investigations which lead to correct diagnosis and appropriate treatment.
Our first patient, K.S., 40 years, salesman, reported to the ENT department because of abundant secretion from the external auditory meatus. After routine ENT examinations (otoscopy, RTG of mastoid and audiometry), an explorative trepanation of middle ear was performed because of the discrete eardrum perforation in the vicinity of which was the site of suppuration. Operative finding showed intact ossicula without infection of the middle ear structures but with a fistulous opening at the anterior wall of the external auditory meatus in the vicinity of the eardrum perforation. Then the maxillofacial surgeon with a more detailed anamnesis obtained a fact that the patient was treated two years previously for the double lower jaw fracture, with fracture lines in the mental region and in the right mandibular collum. Ortopantomography and CT scan showed a bone sequester eg. osteomyelitic focus of condylar processus of that side. Only this localization of bone sequester explains why conventional roentgenograms because of the superposition did not allow clear visibility.
Our second patient, P.R., 55 years, retired, reported to the ENT department with intensive suppuration from the external auditory meatus, large tender swelling and inflammation of the right parotid region. After otoscopy and microaspiration, presence of a fistulous opening at the anterior meatal wall with intact eardrum was established. Because of the swelling and inflammation of the parotid region, this suppuration was connected with purulent parotitis.
Palpation of the tender swelling in parotid region did not show signs of fluctuation, but desiring to help the patient, preauricular incision was performed. This procedue did notempty the collection of puss but formed a salivary fistula. All the time massive antibiotic therapy was conducted without signs of improvement. Suppuration from the ear persisted.
Maxillofacial surgeon included in the team obtained anamnestical facts that the patient had a long lasting toothache of the right upper jaw with constant trismus. Subsequent orthopantomogram showed periapical changes of the wisdom tooth of that side. Ultrasonography of the right parotid space showed not a purulent parotitis but rather a formed puss collection of the right pterygomandibular space.
Discussion
In our first patient, where the cause of suppuration from the ear was an old osteomyelitic process as a consequence of a lower jaw fracture, after condylectomy and hyperoxygenation in baro chamber with antibiotic treatment, rapid healement ensued. This complication of lower jaw fracture with osteomyelitis and spread of the infection toward the ear shows that a precaution is necessary in a priori acceptance of the attitude that high collar fractures should be treated conservatively. Of course, we uphold this attitude in principle. Justification for the oversight of the presence of condylar sequestration are rare localization with difficult RTG diagnostics because of the superposition. We obtained correct diagnosis only with CT imaging. In our second patient, after extraction of the tooth and extraoral incision with retroangular approach, swift emptying of puss collection ensued, suppuration from the ear stopped, trismus and right parotid region swelling receded. In this patient, insufficiently precise anamnesis led the diagnostics in the direction, first of the inner ear disease and then of the parotid salivary gland disease, completely masking the dental origin of the infection.
Only ortopantomography and ultrasonography of parotid region showed the dental origin of the infection with puss collection in pterygomandibular space.
Conclusion
In both our patients symptomatology indicated ear pathology. It is certain that the suppuration from the ear is the most common symptom of purulent middle ear infections. Sometimes, in practice, cases are encountered for which the team work of an otorhinolaryngologist and maxillofacial surgeon with cooperation of a radiologist is indispensable. We emphasize that imprecise anamnesis, biased interpretation of symptoms with crude roentgenographic diagnostics, leads to wrong diagnosis and inadequate treatment.
![]()
Case Reports
Several other patients.

Chemodectoma.
![]()
Osteofibroma.


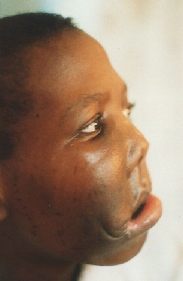
Notice the scars made by the traditional healers.
![]()
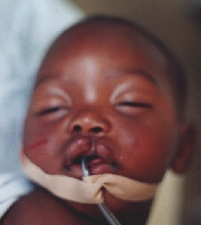
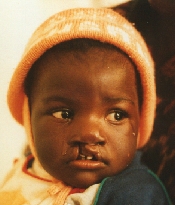
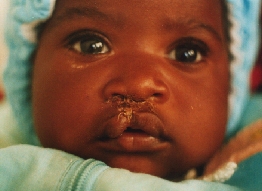
Incomplete cleft lip.

Repair done with Millard I operation.
![]()
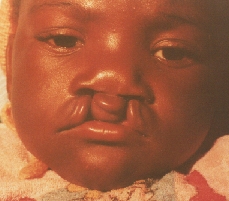
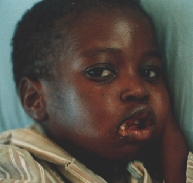
Double complete cleft lip.
![]()

Left parotid abscess.


![]()
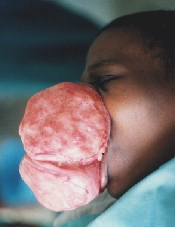
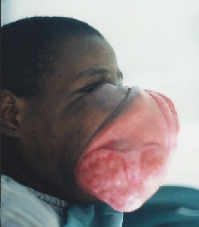
Incipient noma.
![]()

Fully developed noma.
![]()

Injury in a road traffic accident.
![]()

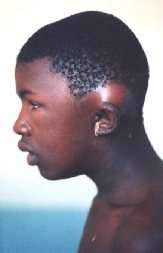
Zygomatic abscess.
![]()

State after the amputation of the nose destructed
by the basocellular carcinoma.
Recurrences on the right eyelid and left
edge of the defect are visible.

![]()

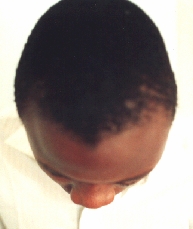
Bone hypertrophy of the LT frontal bone.
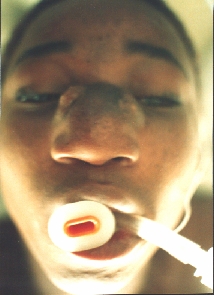
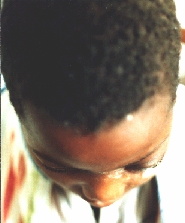
![]()
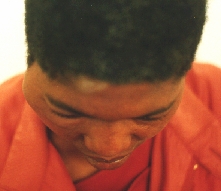
Mastoid abscess. Notice the pus dropping
on the chest.
Treated with cortical mastoidectomy.

![]()
Dermoid tumour.
![]()

Zygomatic abscess.
![]()

Traumatic amputation of the RT nasal ala.
Repaired with composite graft from the
ear.

![]()

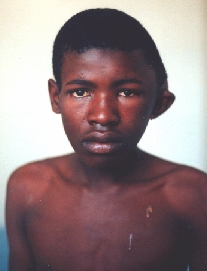
Nasopharyngeal carcinoma with bilateral
neck metastases undergoing (unsuccessful) radiotherapy.
The patient appeared while pregnant so
the radiotherapy was postponed after the delivery.

![]()

State after irradiation and total laryngectomy
for laryngeal carcinoma.
Large pharyngeal fistula with necrosis
of neck tissues.
![]()

![]()

Recurrence of the laryngeal carcinoma.
![]()

![]()

![]()
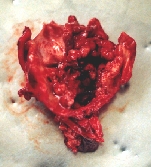
Larynx specimen with the carcinoma involving almost whole of the larynx.
![]()


![]()
® Copyright, 1998. All
Rights Reserved.
SigmaMax Publishing.