
|
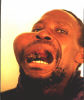
Large exulcerated parotid salivary cystadenocarcinoma.
Notice right ophthalmoplegia.
|

|
The tumor was removed. Neck was macroscopically clean.
The wound was sutured primarily. However, the patient slowly went to a coma
and passed away seven days after the operation.
|

|
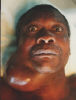
Large bleeding, exulcerated, necrotic parotid
tumor.
|

|
The tumor was removed. Neck was macroscopically clean.
However, the patient succumbed several hours after the operation. Death was
attributed to large preoperative and intraoperative loss of
blood.
|

|
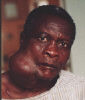
State after left hemimandibulectomy with exarticulation.
Notice the deviation of the mandible to the left.
|

|
This patient had a large, exulcerated carcinoma of the
retromolar trigone involving the inner face of the mandible and anterior
tonsillar pillar and the tonsil. Notice a dexon suture that was inserted to
appose the sides of the defect.
|

|
The patient was referred to postoperative radiotherapy
and re-appeared several years later with a large recurrence involving the left
parotid gland, the defect after left hemimandibulectomy, extending to the left
buccal sulcus. Radical parotidectomy was performed but the patient developed a
recurrence after several months with brain involvement. He was lost from the
follow-ups - presumed dead.
|

|
State after the removal of a left zygomatic and lower
palpebral tumor. Notice the prominent scar and the ectropion.
|

|
Carcinoma destructing the nose and extending per
continuitatem to the upper lip and submandibular regions on both
sides.
|

|
Debulking was done and the patient was referred for
radical radiotherapy. He passed away after several weeks and the cause of
death was never reliably established. No distant metastases and other diseases
were found on post mortem.
|

|
Large exulcerated necrotic carcinoma destroying the body
of the mandible on the left side.
|

|
The tumor was removed and only very narrow and thin piece
of the cortical bone was left on the lower mandibular edge to preserve the
space.
|

|
The wound was closed primarily with one neck flap closing
the postoperative defect while the other closed the defect after elevation of
the first flap. The patient was irradiated, attended regularly follow-ups and
does not have any signs of local recurrences or distal
metastases.
|

|
Epulis - gigantocellular mandibular tumor. Removed with a
blade and a cautery and the defect left to granulate per secundam
intentionem.
|

|
The patient had a history of undergoing an orbital
enucleation due to a long-standing infection.
|

|
Carcinoma was removed from the orbital defect and
something that looked like a shrunken eyeball.
|

|
It is unknown where the previous operation was done and
what was the histology.
|

|
The patient was referred for radical
radiotherapy.
|

|
However, she did not complete the radiotherapy and did
not attend follow-ups.
|

|
Several weeks later she appeared with a recurrence in the
temporal region. She refused all further management and is presumed
dead.
|

|
Parotid tumor. A biopsy (sic!!!) was done in a missionary
hospital in rural areas.
|

|
Since the histology was a cystadenocarcinoma a partial
parotidectomy was done. Operation lasted at least one hour longer because the
scar and the skin surrounding it had to be dissected with the
parotid.
|

|
CT scan showed a tumefaction in the upper nose, ethmoid
and frontal sinuses, and a fist-size lesion in the anterior
lobe.
|

|
During the initial operation huge black masses were
removed through an external rhinotomy approach. Subsequently, the neurosurgeon
removed the brain tumor.
Histology: Blastomycosis.
|

|
Maxillary sarcoma.
|
|
Total maxillectomy was done.
|

|
Maxillary sarcoma.
|

|
Total maxillectomy was done.
|

|
The patient did not appear for
follow-ups.
|

|
|

|
Six months later he appeared with even bigger
tumor.
|

|
Another extended maxillectomy was done.
|

|
The patient did not appear after that and is presumed
dead.
|

|
|

|
Total laryngectomy was done for laryngeal carcinoma.
Pharyngeal fistula.
Department of Otorhinolaryngology,
Clinical-Hospital Center Zemun, Belgrade.
|

|
Fistula was closed with the Ariyan's
myocutaneous flap.
|

|
Bakamjian's deltopectoral flap was elevated
to facilitate elevation of the Ariyan's flap and to preserve it for
possible future use.
|

|
In the immediate postoperative course the flap showed
signs of venous stasis so the patient underwent a course of hyperbaric
oxygenation.
|

|
Terminal stage of the laryngeal carcinoma. Local
peristomal recurrence, pharyngeal fistula with a gastric tube in
place.
|

|
Plasmacytoma.
|

|
Undergoing radiotherapy.
|

|
Radiotherapy was unsuccessful. The tumor did not show any
signs of regression. The patient was referred to chemotherapy but without a
favorable response.
|

|
A newborn infant in the incubator in ICU. Succumbed
during the first week.
|

|
Ameloblastoma before the first operation.
|

|
One year later the patient was again operated on for
recurrence. Subsequently, the maxillofacial surgeon did a hemimandibulectomy
approximately two years after the first operation.
|

|
Carotid body tumor - chemodectoma. The patient was HIV
positive and had a small child. Therefore, only an observation was
done.
|

|
Osteofibroma. 10-years history.
|

|
The patient was functioning normally.
She used to cover her face with a scarf.
She did not give any explanation why she did not visit the doctor for such
a long time.
|

|
However, numerous scars on the skin above the tumor imply
that she was treated by a natural healer.
|

|
Major problem was intubation which was achieved
successfully by the anaesthesiologist.
|

|
No further cosmetic intervention was deemed
necessary.
|

|
Incomplete cleft lip.
|

|
Millard I operation.
|

|
Bilateral cleft lip.
|

|
Millard I operation was done on one side.
|

|
And then on the other side.
|

|
Maxillary carcinoma.
|

|
Subtotal maxillectomy was done.
|

|
Parotid abscess.
|

|
Drainage was done through a parotidectomy
incision.
|

|
Obvious improvement after surgery and systemic
antibiotics.
|

|
No further intervention was necessary.
|

|
Incipient noma.
|

|
Fully-developed noma.
|

|
Partial avulsion of the auricle sustained in a road
traffic accident.
Secondary suture was done with excellent results.
|

|
Zygomatic abscess.
|

|
Resolved after drainage and systemic
antibiotics.
|

|
Carcinoma of the nose.
At initial presentation the nose was already almost completely destroyed
by the tumor.
|

|
Basically, only a completion amputation was done. First
recurrence appeared after 14 months and was duly removed. Since then, during
some 7 years, the patient underwent several removals of local
recurrences.
|

|
CT showed bone formation in the lateral floor of the
anterior cranial fossa and upper and lateral bony orbital
walls.
|

|
The patient was referred to Harare for further
management.
|

|
Mastoid abscess.
|

|
Cortical mastoidectomy was done and systemic antibiotics
given.
|

|
Full recovery ensured as expected.
|

|
Saddle bag shaped fibroma on the nasal bridge.
Management was delayed because a possibility of a meningo- or
encephalocele could not be ruled out in another institution.
|

|
Zygomatic abscess.
|

|
|

|
Exulcerated necrotic parotid tumor.
|

|
Histology: cystadenocarcinoma.
Parotidectomy was done.
|

|
Ludwig's angina.
Almost fully recovered with large doses of IV antibiotics.
|

|
Defect of the nasal ala inflicted by human
bite.
|

|
The patient was dressed regularly with Betadine.
The ensuing scar was barely noticeably so further treatment was
unnecessary.
|

|
Nasopharyngeal carcinoma with bilateral neck
metastases.
|

|
Since the patient was pregnant radiotherapy was postponed
after delivery.
Response to radiotherapy was minimal. Presumed dead.
|

|
Laryngeal carcinoma.
Necrosis after total laryngectomy and radical postoperative radiotherapy.
|

|
Laryngeal carcinoma.
Large defect after surgery and radiotherapy.
|

|
Laryngeal carcinoma.
Peristomal recurrence.
|

|
Laryngeal carcinoma.
Pharyngeal fistula.
|

|
Laryngeal carcinoma.
Pharyngeal fistula.
|

|
Laryngeal carcinoma.
Larynx with tumor removed.
|

|
This tumefaction resembled ameloblastoma.
Several
biopsies were inconclusive.
During operation major bleeding from the base of the skull was arrested
only with several packets of bone wax.
|

|
Wound secernation was present for several years after the
operation.
Re-operation was not done due to fear of another bleeding.
|

|
"Dirty" wound with defect of the upper
lip.
|

|
The wounds was dressed with Betadine regularly during
several days.
|

|
Finally, a debridement was done. Reconstruction was
performed with a transposition flap from one side of the nose and rotation
flap from the other.
|

|
Upper lip is now elongated because too much tissue was
transposed in the defect.
|

|
Anotia.
|

|
Parotid cystadenocarcinoma.
Parotidectomy was done.
|
|
Submandibular cystadenocarcinoma.
|

|
Radical exenteration was done on at least three occasions
in the last seven years.
|
|
Another very suspicious lymph node appeared in the buccal
region.
|

|
However, the patient refused any further
management.
|

|
Large exulcerated submandibular salivary
tumor.
|

|
The patient was subsequently operated on. Macroscopically
the neck was cleaned of tumor. However, the patient did not appear for reviews
and several months later came with an inoperable neck recurrence and
subsequently passed away.
|

|
Notice scars after scarifications done by a traditional
healer.
|